We meant to ask about prenatal vitamins. Nelly has been taking these gummies that are overly sweet and she has to chew and she can't stand them anymore. The next thing we said was going to be, "do you have any recommendations for prenatal vitamins?"
But I don't know what we did actually say next, because that's when the NP told us the yolk sac was 9mm.
That datum meant nothing to us, either.
Five weeks earlier, just three days after we learned about the pregnancy, sitting six hours in a covid-infested emergency room with a sharp pain in her left abdomen, was the first time I learned what a yolk sac was. It was the thing we needed to see in the uterus where it was supposed to be to know that this pain wasn't what it wasn't supposed to be. It was that thing that finally showed up in the ultrasound, a tiny round black and white bubble that the radiologist labeled without further comment "Yolk Sac", that meant the pregnancy was not ectopic, that we could stop worrying, that we could relax and wait the remaining six hours until a doctor finally saw us to tell us the baby was fine.

There are very tight bands on the proper size of the yolk sac, our NP explained. Outside of the range 2-5mm could indicate genetic aberrations and early loss of pregnancy (see Detti et al 2020b)
My son, Ezekiel, who is the correct length with a strong heart rate of 177bpm, was just wriggling and squirming around on the ultrasound for us. We saw him move his hands with the finger bones just showing, rolling over like someone with a noisy neighbor trying to get back to sleep. He was perfect.
 |
| still shot of Ezekiel at 10wks gestation; in videos, he is sucking his thumb, quite unconcerned with his yolk sac |
According to the medical literature (or at least this article from 2005), the largest yolk sac associated with a live birth that is recorded in the medical literature was 8.1mm. Ours is 9mm. The case of the paper involved a woman with a bicorneate uterus (which I had to look up), and the large yolk sac may have formed as a compensation for the uterine structure. These researchers suggest it is the quality and not the size of the yolk sac that is important.
When you learn you're having a baby, you make plans in your head of what your child is going to be like.
Of course I've wanted to have a son. But at one point before we found out his gender, we strongly suspected the child might be a girl. And I formed thoughts in my head of tea parties at little miniature tables with adorably tiny cups, of cute pink dresses and red ribbons, of holding her on my shoulder on walks. And when we learned it was a boy, of course I was happy. But also I was sad. Because I had started to love that little girl I had dreamed up. And that little girl wasn't going to be there.
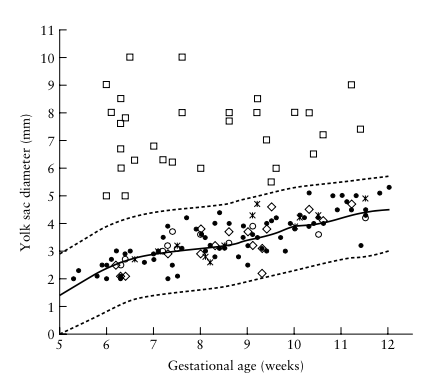 |
| from Angiolucci et al 2011. squares are enlarged yolk sacs. all observations ended in miscarriage |
You may be wondering, as I was, what the size of the yolk sac has to do with Down syndrome in the first place. It's not like the big hulking yolk sac is going to suck up the good genetics out of the baby, until all that's left is the stuff with triplicate copies.
They are only confounded, and the common cause is genetic aberration. If there is some deviation in the genetics from the normal 46 chromosomes, then the same genes developing the baby also develop the baby's yolk sac. So if there is aberration in the yolk sac, there is likely also aberration in the baby. The share a likely common cause.
When you see that the yolk sac is large, outside the range of 5mm, maybe even as large as 9mm, you are seeing smoke from the fire. The same fire can also lead to an early loss of the pregnancy or to abnormal genetics. That's how these things all connect.
Many trisomies are not as benign as Down syndrome. Many are incompatible with life. The little one develops anatomy in the wrong locations, pieces of the face fail to come together, there are holes where there oughtn't be, the brain is reduced in size or fills with fluid. Little Ezekiel was whole, entire, with a giant brain-filled head, adorable little hands and feet that he could move and cross at the ankles. Little Ezekiel was taking a nice baby nap until that rude sonogram disturbed him, he waved at the camera, and then we went back to sleep. My son did not have any trisomies that are incompatible with life.
We were at 10.4 weeks, which is a little late to be called "early pregnancy", but still too early to not be called "early pregnancy". Studies of yolk sacs take place in early pregnancy, because after 10 weeks the thing is supposed to start to disappear (and not grow to 9mm). By 12 weeks it should be entirely gone. So there are no studies focused on the correlation of yolk sac diameter and baby health specific to 10-week fetuses. They all relate to "early pregnancy" generally, from 5 weeks to 10 weeks, which is perhaps important because the yolk sac grows by as much as 0.4mm/week since it first appears. This steady growth rate actually allows use of yolk sac diameter to predict gestational age. If studies make no distinction between 6mm yolk sac at 6 weeks and 6mm yolk sac at 10 weeks, and they are instead just "6mm yolk sac", then that seems to be missing some key information. The 6mm/10wk yolk sac might have originally been 2.8mm at 5 weeks, which is close enough to normal to not be a major worry.
9mm at 10 weeks though?
The first time we saw Ezekiel, we couldn't actually see Ezekiel. He was still inside the yolk sac and was too tiny to see. We didn't know he was a boy yet. But we did see him (not literally "see", since this is reflected sound), and we saw his yolk sac, and there was nothing about the yolk sac that was cause for concern. The sonographer wrote that all was normal. But she didn't record any measurements, either. Maybe we could have seen it then, if we'd actually measured, that rather than a normal 2.8mm, the yolk sac was actually a dreaded 3.1mm... easy difference to miss when you're not using calipers.
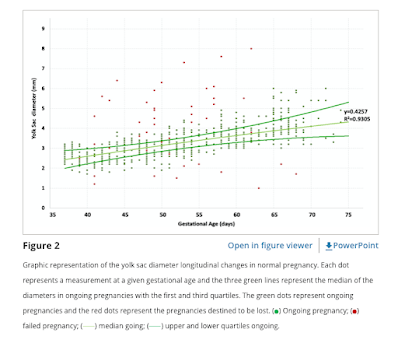 |
| from Detti et al 2020b |
And what they found is that large yolk sac is a marker for early pregnancy loss, but when it is a marker for early pregnancy loss it is detectable as a marker from very early on. To put this differently, if there is a genetic aberration that will result in miscarriage, it will cause irregularities in the baby and the yolk sac, and the irregularities it causes in the yolk sac appear very early. There were no irregularities in our yolk sac at 5 weeks. When the study saw cases of a large yolk sac at 10 weeks, the rate of miscarriage was essentially the same as the control (actually smaller, but small number stats).
Here is what they have to say of their findings:
After 5 complete weeks of gestation, the YS reliably detects pregnancies destined to be lost, also confirmed by multivariate analysis. In pregnancies destined to fail, the YS was either smaller or larger than in pregnancies continuing beyond the first trimester. While all pregnancies with a large YS were lost within 10 weeks, some pregnancies with smaller YS were lost beyond 10 weeks of pregnancy. The etiology of a large YS is essentially unknown, however 18–66% of large YS diameters greater than 5–6 mm have been associated with abnormal karyotypes21,22. Our limited genetic results seem to corroborate these previous findings.
[...]
In conclusion, we were able to establish a statistical model using only early pregnancy ultrasound markers to predict a first trimester loss. GS and YS were the earliest parameters that could reliably be used as prognostic factors for pregnancy loss, as they became abnormal as early as 6 weeks of gestation with high sensitivity and specificity. Of all the evaluated parameters, the YS was the strongest single predictor. These findings are clinically useful for patient counseling and determining the need for closer monitoring. In fact, if these parameters are normal at 6 weeks, the pregnancy will likely continue beyond the first trimester. Although needing prospective validation, our results support changing the current standard of care of performing the first obstetric ultrasound at 9 weeks of gestation to 6 weeks of gestation. If the YS and the GS are normal, a provider can offer reassurance concerning the decreased likelihood of a pregnancy loss.
So what does it mean, for us, at 10.4 weeks, with an apparently healthy baby the correct size, correct heart beat, mild subchorionic hemorrhaging, and an enlarged yolk sac of 9mm?
It might mean that we're "over the hump" of worry. It might mean we can relax, be still, knowing our baby has continued growing and thriving regardless of his dumb old yolk sac there. Some other studies confirm this, such as Cho et al 2006. They found that very large yolk sacs might exist in normal pregnancies -- however, "very large" here meant 6mm, not 9mm. All the same, I feel reassured that I will be able to meet my son in a few months.
So what is my son going to be like?
Here's one study (Gersak et al 2012):
Methods: Retrospective analysis of 42 patients with no history of diabetes between 6 and 12 weeks of gestation with increased yolk sac diameter measuring ≥6mm was evaluated by transvaginal ultrasound. Sonographic findings were correlated with karyotype. The Fisher’s exact test and exact conditional logistic regression analysis were used for statistical analysis.
Results: Chromosome abnormalities were found in 76.2% of chorionic villi samples. [...] None of the patients with a yolk size diameter ≥8mm and viable pregnancy had a normal karyotype. [...] Nine patients with viable pregnancy had a yolk sac ≥6mm (six patients with normal karyotype, one patient with monosomy X, one patient with trisomy 16, and one patient with trisomy 21).
Conclusion: Our data indicate that enlarged yolk sac may also be visualized in viable pregnancies. Patients with an enlarged yolk sac and normal karyotype require detailed ultrasound evaluation in the second and third trimester.
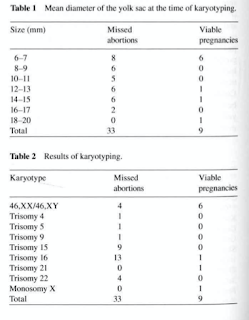 |
| Gersak etc 2012 |
But whatever the problems with the study, it's not great news.
Children with Down syndrome can lead full, happy lives. They laugh, play, learn, and grow. They can grow up to hold jobs, live semi-independently, and otherwise be healthy members of society. They will struggle with bullying and nonacceptance, more than other teenagers. But they aren't hopeless.
You imagine your child a certain way, though. You make dreams of how they'll be, things they'll say, how you will interact with them. You imagine them growing up and the sequence of life events that takes place, from the first day of kindergarten through high school and their eventual wedding.
So it's heartbreaking to consider losing all that happy life.
And it makes you want to cry, and even mourn. But it's not the end of all happy life. Just that particular happy one you envisioned. There can still be a different happy life.
Hearing my son was my son, and not the daughter I pictured tea parties with, I also wanted to mourn. I lost something I had fallen in love with. But that doesn't mean I'm not ecstatic for my son, and that I'm not excited for the tree climbing and sword fighting to come.
I don't know how my son will be. I have faith in God, whatever the outcome, and know the Lord of all the earth will do right. He alone holds the power of life and death, and man's power is nowhere so manifestly impotent as when he is scrolling through library archives looking for any glimmer of hope that might mean his son will live. I do not have faith that everything will work out pleasantly the way I want it to, because I know better than that; but I have faith that God will do right.
And yet, I am prepared to learn that those three minutes on the ultrasound, seeing him wriggle and suck his thumb, will be the only time I will get to share with him. They were a good three minutes. I will be thankful for them.
We submitted blood for a non-invasive genetic test, but even then how do you interpret results? If it says negative with 98% certainty, but you're in a 66% positive category, is it actually negative with 98% certainty?
We won't have the results until between 2 and 7 days, which is not a great window of time for uncertainty. The next ultrasound is in two weeks. I'm writing this to gather my thoughts as I await the results. Based on what I saw in the ultrasound, based on the poor quality of the truly grim studies and the less grim nature of the better quality studies, I think --- think as opposed to hope --- I think my son will make it, the yolk sac was mis-measured or something equally as erratic, he'll come out healthy, and I actually doubt he will have any kind of trisomies. He'll set a medical record (9mm > 8.1mm!) and I'll make sure the NP puts that into writing for the medical literature -- healthy baby, normal karyotype, 9mm yolk sac at 10.4 weeks.
Hopefully the next person with the same bizarre convergence of edge cases, scrolling through search results like me, can read this one day and sleep a bit better.
But for now, waiting, all I have to really offer is the studies I found and the conclusions I took from them.
If you are very early (5-8 weeks, say), unfortunately the statistics are not good. You are likely to lose the pregnancy. Of course "likely" is talking about trends in many, many instances; for any given person, it is always either 0 or 1. It is always either yes or no, do or don't, and the probabilities we throw out are just ratios of those 0s and 1s. Whatever the percentages are, who knows what your individual case will be. Why ensure the worst possible outcome yourself, when you don't know which side of the coin you'll actually fall on?
If you are in our case, if everything looks fine, and has looked fine, but this one single thing caused your medical provider to sit you down and express concerns, then things might not be as bad as they sound right now. You might be over a hump and are in the same statistical space as pregnancies without large yolk sacs.
Don't take away the wrong message. A large yolk sac is a cause for concern. Depending on your gestational age, it could be a very big cause for concern. But it's not a death sentence. And it's maybe not as bad as you're fearing. It's easy to be scared when the person in the white coat tells you bad news, but don't let it impact your judgment.
This was originally written in January of 2022, when my son Ezekiel was just at around 11 weeks gestation. I wrote it largely to collect my thoughts on the articles I was reading and avoid stumbling on the same article over and over in search results. It was a kind of annotated bibliography that became overly personal. I left it off to finish my PhD dissertation (in physics, completely unrelated to embryology). I have edited it to add references and clarifications. Today it is more than two weeks since Ezekiel's birth. He is perfect. Soli Deo gloria.

Here are some of the articles I looked at, with comment:
- Goldstein et al 1996: begins with 102 women with confirmed miscarriages ("early pregnancy failure"). They found that 43% of these miscarried embryos has abnormal genetics ("karyotype"=DNA pattern), and 18 of the 102 miscarriages had large yolk sac, but no correlation of large yolk sac with abnormal karyotype.
- Kucuk et al 1999: looks at 250 pregnancies. Of these 250 pregnancies, 219 ended in a viable child and 31 ended in embryo demise. Also of these 250, 28 had enlarged yolk sac. Of those with enlarged yolk sac, 20/28 (71%) died in utero. I can't actually find any methodological faults in this study.
- Angiolucci et al 2011: performed ultrasounds on all women in a hospital, but focus only on those with early pregnancy loss, limiting to 156 observations. Of these, 30 had an enlarged yolk sac, and then 28 of those with enlarged yolk sacs had abnormal genetics. But that 28/30 is conditioned on the embryo having died in utero, and early pregnancy loss is already correlated with abnormal genetics. So among a population with high rate of abnormal genetics, embryos with large yolk sacs have a high rate of abnormal genetics.
- Gersak et al 2012: begins with 42 patients between 6 and 12 weeks gestation with enlarged yolk sac (more than 6mm). Of these 42 pregnancies, 33 ended in miscarriage ("missed abortion" = a miscarriage without cramping or other symptoms). Breaking the 42 observations into smaller bins of size (eg 6-7mm, 8-9mm, etc.), the miscarriage rate is always at least 88%. Unlike the others, this retrospective study begins with large yolk sac rather than beginning with miscarriage.
- Salamanca et al 2013: begins with 200 miscarried embryos before 10 weeks, of which 104 embryos had abnormalities. Finds, among miscarried embryos, that normal yolk sac size and shape are correlated with normal morphology. This is, again, conditioned already on the embryo having died in utero, which is itself linked to abnormalities.
- Ashoush et al 2016: begins with 204 women with confirmed miscarriages, and establishes a link between abnormal yolk sac morphology and abnormal embryo morphology. But this is again conditioned already on the embryo having died in utero, which is itself linked to abnormalities.
- Saguna and Sukanya 2018: looked at 500 pregnancies. Found that abnormal yolk sac shape was a strong predictor of poor pregnancy outcome, but that yolk sac size was not a strong predictor. Similar methodology as Kucuk et al 1999 above, which I don't find any fault in, but contrary result.
- DeVilbiss et al 2020: looked at 617 women, of whom 64 had early pregnancy loss. Found various features such as low heart rate and small size were predictors for pregnancy loss; but abnormal yolk sac size was not a valuable predictor of pregnancy loss.
19 comments:
I first thought your original post was from August 2022 and then it makes such tense reading. So very happy that your post was from January 2022 and that your son is born and well. Congratulations to both of you !!
I have just had a pregnancy loss where a large yolk sac was found and just stumbled across this blog as I was searching the web for some more information. I'm so glad to see your little son was born healthy and happy. A life time of happiness to you all x
I'm so sorry to hear about your loss. It was painful even just writing this blog post and remembering how the worry felt. I hope you never have to go through it again.
Thank you for writing this article. I found out I have a large yolk sac and am trying to absorb everything. After a history of losses, our baby is measuring on track but I'm terrified of something going wrong. I appreciate your thorough analysis here.
Thank you for writting this. The internet is a scary please. It is easy to loose faith. Blessing for your little one.
I was just told I have a YS of 8mm at 10.5 weeks. A very similar case to yours, healthy as can be otherwise. Thank you for this blog, this is the only positive and most informative thing I’ve read today. I am so happy your baby boy is healthy! You’ve given me hope. ♥️
Hi Anonymous, I'm sorry you got the same scary news. My wife and I are praying for your baby. I hope everything goes well and it's only a false alarm.
Thank you for providing such useful information all together! I have a YS that measured 5.4mm at 7 weeks and 6.4mm at 8 weeks. GS and embryo size / HR are as expected. Both USG and OB doctors didn't mention anything about the YS size though, I just came across this accidentally over the internet and now I'm trying not to freak out and searching for information that may help us to predict what our real chances are, and this post is the more realistic that I could find. Just praying for my miracle at this point.
Congratulations on your little boy!!
God bless you and your family. U gave me hope as our YS is measuring 6,9mm at 6,5 weeks and stil no heartbeats.
Hi! I’m not sure if you’ll see this, but was just wondering how you’ve been making out. We just got the news about an 8mm YS today, baby is perfect otherwise. We got the blood draw for genetic testing and are in the waiting now.
We just lost our pregnancy at 8 weeks, with, as you could suspect, a large YS. This article was a great help, thank you so much for it. I'm glad to see that your son turned out to be a healthy, beautiful child. I just wanted to thank you for all this information.
Our son also had an enlarged yolk sac, albeit not as large as in your case. Thank you for writing this blog. It brought me great comfort at a time of turmoil and confusion. He is now ten days old and wriggling happily at my side as I post this. Blessings to you and your family. Soli deo gloria.
Thank you so much for sharing your story! God bless! My partner and I really needed to read this. We are so happy everything turned out well and you got to meet your lil wonder ♡ Had our scan today at 10w, measuring 10+6 with a yolk sac of 10mm. Praying and hoping for a happy outcome. To setting another record! 🙏
Thank you for this article. Just found out are baby passed away on our ultrasound scan today. Had a low heart rate last week of 103. The yolk sac measured large last week and appeared large again this week. Baby should have been 7 weeks today but measured only a lil over 6. Such a helpless feeling to wait and see what happens. I really appreciate all the info here it has given me some peace amidst all the uncertainty.
God bless you and your lil one! So happy he is healthy. 🫶🏻 Every good thing should be celebrated in this world that can be so hard sometimes.
So your son was born without any genetic abnormalities? I’m struggling over here and need to know for sure how this turned out for you. Thank you.
Ezekiel is 2. He has no genetic abnormalities. His only medical condition is a clogged tear duct. He is bilingual and can count to six in two languages. He can climb a playground ladder (with minimal help from dad).
However, and I wish this were more clear in the blog post, with yolk sacs, weeks matter. We found a large yolk sac at week 10, and everything else was fine. The case of discovering a large yolk sac at week 6 carries a lot more risk of miscarriage. The paper I cited tracking yolk sac size suggests large yolk sacs by a specific week have high risk of loss within a few weeks, while large yolk sac size after a certain week is irrelevant.
All said, a risk is a ratio of 0s and 1s. Your case might be one of those 1s.
I can say that much as a scientist outside his field based on the statistics of some studies.
Meant to add this (typing while trying to make breakfast)
As a scientist, I can say that much.
As a dad, I am very glad we did not listen to the midwife when she suggested we consider termination. Losing our boy would have been the worst possible outcome… why would we have done that ourselves?
I have a lot of anonymous comments (which is fine!) but I can’t tell if a new anonymous is an old anonymous. When we received the news, we had normal heartbeats and a healthy ultrasound. At the next ultrasound the providers didn’t even look at the yolk sac, because they were no longer worried. I dunno where you are or what your signs are.
It’s possible to have a large yolk sac and nothing else is wrong. That was our case. But in our case, we saw that nothing else was wrong. We would have still made the same decision, but looking at all the data made us feel better about it.
I’m also very curious how this turned out, my husband and I are in the same boat.
I want to first say how much I appreciate the effort you put in to reviewing the research. Finding your story has been so helpful. The past two days have been so confusing. We’ve done about 4 earlier ultrasounds which all had normal yolk sac measurements. And then this week around 10.5/11 weeks we had an ultrasound where they told us the yolk sac was enlarged at 8.5mm. Baby’s growth and heart rate are both incredibly normal/strong. Our NIPT testing all came back low risk, but they’re worried about trisomy 22 or another rare chromosomal abnormality not tested by Natera’s NIPT testing. They’re referring us to a fetal maternal medicine specialist. I’m curious, did y’all do additional testing other than NIPT? We live in Idaho which is a fairly small state, so I’m wondering how much of their concern is due to just never having seen an enlarged yolk sac before.
Post a Comment